 Skip to content
Skip to content

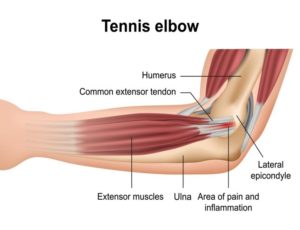
Lateral (outside) Epicondylitis ‘Tennis Elbow’
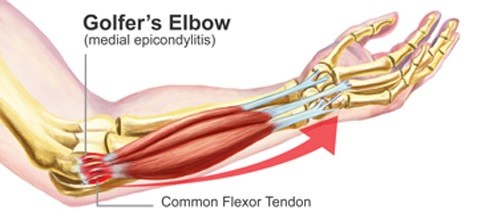
Medial (inside) Epicondylitis ‘Golfers Elbow’
Epicondylitis is a painful condition that occurs when tendons either on the outside or inside of your Elbow are overloaded. This usually occurs via repetitive activities of the wrist and/or forearm.
You don’t have to be an athlete to experience epicondylitis, often painters, carpenters, and desk workers with typing and repetitive use of a computer mouse or keyboard can cause the same tendon irritation. This type of condition is often recognised as a form of RSI (Repetitive Strain Injury)
Outside Elbow
Inside Elbow
Many of the muscles that exert movement and strength in the forearm, wrist, fingers, and thumb originate on the forearm / Elbow. If you watch your forearm whilst moving your wrist or fingers up and down, you will see muscular movement/activity in the forearm area (front or rear).
The outside (thumb side) of the elbow provides a large communal (group) tendon for many of the extensors of the wrist and fingers. The inside (small finger side) of the elbow provides a large communal (group) tendon for many of the flexors of the wrist and fingers.
Symptoms
The symptoms of epicondylitis (tennis/golfers’ elbow) develop gradually. In most cases, the pain begins as mild and slowly worsens over weeks and months. There is usually no specific injury associated with the start of symptoms.
Common signs and symptoms of tennis elbow include:
- Pain or burning on the outer/inner part of your elbow
- Weak grip or wrist lifting strength
- Sometimes, pain at night
- Occasionally nerves may be irritated and cause pins & needles or numbing sensations below the elbow.
- In extreme cases, inflammatory swelling may be observed.
The symptoms are often aggravated with forearm & wrist activity and can be noticed quickly via simple daily activities like, picking up a pot or kettle, twisting a jar lid, or shaking hands. Your dominant arm is most often affected; however, both arms can be affected.
Classification / Types
Epicondylitis is usually diagnosed into different types (Type I, II or II) by practitioners. The type indicates the fibre type involvement and the proximity of involved tendons insertion (anchoring) point.
Risk factors
Factors that may increase your risk of tennis elbow include:
- Age. While tennis elbow affects people of all ages, it’s most common in adults between the ages of 30 and 50.
- Occupation. People who have jobs that involve repetitive motions of the wrist and arm are more likely to develop tennis elbow. Examples include plumbers, painters, carpenters, butchers and cooks.
- Certain sports & training. Participating in racket/bat sports increases your risk of tennis or golfers’ elbow, especially if you employ poor stroke technique. Weight training if practised with poor form can also easily initiate this condition.
- Other repetitive activities e.g., playing musical instruments, DIY, gaming, knitting and even extensive mobile phone usage can lead to this condition forming.
If ignored for too long then this type of condition can expand to aggravate local nerve tracts, other neighbouring muscle chains as also local joints (including other soft tissue structures around the joints). This can lead to symptoms being caused to potentially expand to the wrist, fingers, shoulder and even the neck.
Treatment
Early-stage epicondylitis can improve on its own provided aggravating factors are mitigated against.
If, however, over-the-counter pain medications and other self-care measures such as stretches aren’t helping, you may want to see a Physiotherapist or Osteopath.
- Mild cases may be approached with icing, guided stretching, and a specific exercise routine stressing the tendon eccentrically to assist in the body’s natural ability to heal.
- Taping techniques and elbow clasps may also assist with a relatively early-stage condition of this type although these are often not a permanent resolution.
- Manual therapy (including controlled, slow manipulations) to the local joints may aid in resolving symptoms.
- More stubborn cases can be assisted with Extracorporeal Shockwave Therapy (ESWT) and in some cases Trigger Point Dry Needling for secondary forearm muscle hypertonicity.